Are Deep Squats Bad for Your Knees?
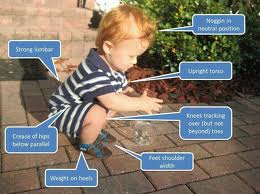 The picture above shows what many people in the fitness industry call a squat. Having a seventeen month old son, I get to see this picture day in and day out. Over the years, somehow the form begins to change and the myth about the proper squat has evolved.
The picture above shows what many people in the fitness industry call a squat. Having a seventeen month old son, I get to see this picture day in and day out. Over the years, somehow the form begins to change and the myth about the proper squat has evolved.
Being a personal trainer and helping people in the health and fitness arena for over 13 year, I always get the same question as it relates to squats.
“I thought (or heard) that squatting below the knees is bad for you? ”
Although I would love to go into my personal and professional experience on this topic, I wanted to mainly dive into what the studies have found. Anyone with knee issues that have not gotten them taken care of will most likely have range of motion limitations so this article is just the fact and what the studies, as a whole, have said.
The history of the myth that squatting below the knee is bad for you
The whole idea that deep squats heighten injury risk can be traced to studies conducted by Karl Klein at the University of Texas. Using a self-developed measuring device, Klein (1961) noted that weightlifters who frequently performed deep squats displayed an increased incidence of laxity in the collateral and anterior cruciate ligaments compared to a control group that did not. Klein concluded that squatting below parallel has a detrimental effect on ligamentous stability and should therefore be discouraged. Soon thereafter, the AMA came out with a position statement cautioning against the performance of deep knee exercises because of their potential for severe injury to the internal and supporting structures of the knee joint.

Research since 1961, however, has refuted Klein’s findings, showing no correlation between deep squatting and injury risk (Meyers, 1971; Steiner et al., 1986; Panariello et al., 1994). In fact, there is some evidence that those who perform deep squats have increased stability of the knee joint. In a study using a knee ligament arthrometer to test nine measures knee stability, Chandler, et al. (1989) found that male powerlifters, many of them elite class, demonstrated significantly tighter joint capsules on anterior drawer compared to controls. Moreover, both the powerlifters as well as a group of competitive weight lifters were significantly tighter on the quadriceps active drawer at 90 degrees of knee flexion than control subjects.
Contrary to Klein’s hypothesis, ACL and PCL forces have been shown to diminish at high degrees of knee flexion. Peak ACL forces occur between 15 to 30 degrees of flexion, decreasing significantly at 60 degrees and leveling off thereafter at higher flexion angles (Sakane, et al., 1997; Li, et al., 1999; Kanamori, et al., 2000). PCL forces rise consistently with every flexion angle beyond 30 degrees of knee flexion, peaking at approximately 90 degrees, and declining significantly thereafter (Li, Zayonz, Most, et al., 2004). Beyond 120 degrees, PCL forces are minimal (Markolf, et al., 1996).
The reduction in ACL and PCL forces associated with deep squatting is believed to be a result of an impingement between the posterior aspect of the upper tibia with the posterior femoral condyles as well as compression of various soft tissue structures including menisci, posterior capsule, muscle, fat, and skin (Li, Zayontz, Defrate, et al., 2004). This helps to constrain the knee joint, significantly reducing anterior and posterior tibial translation and tibial rotation compared to lesser flexion angles. Hence, tolerance to load is enhanced in the deepest portion of the squat with a protective effect conferred to ligamentous structures.
It can be argued that ligamentous injury risk during squatting is actually greatest in the parallel squat-the position where PCL forces are at their apex. However, the magnitude of maximal posterior shear during squat performance (approximately 2700 N) is well below the strength capacity of a young, healthy person’s PCL, which is estimated to exceed 4000 N (Escamilla, 2001). It should also be noted that regimented resistance training confers an adaptive response in connective tissue, increasing its strength capacity (Buchanan & Marsh, 2002). A stronger ligament serves to improve tolerance to load, further reducing the prospect of injury.
The greatest risk for injury during deep squatting would theoretically be to the menisci and articular cartilage (Escamilla, 2001; Li, Zayontz, Most, et al., 2004). Tibiofemoral compressive forces have been shown to peak at 130 degrees of knee flexion (Nisell and Ekholm, 1986) where the menisci and articular cartilage bear significant amounts of stress. Deep squats also may increase susceptibility to patellofemoral degeneration given the high amount of patellofemoral stress that arises from contact of underside of the patella with articulating aspect of femur during high flexion (Escamilla, et al., 2001). However, there is little evidence to show a cause-effect relationship implicating an increased squat depth with injury to these structures in healthy subjects.
Squat depth has been shown to have a significant effect on muscular development at the hip and knee joints, particularly with respect to the gluteus maximus (GM). Caterisano, et al. (2002) demonstrated that while average muscle activity of the GM was not significantly different in both the partial squat (16.92 +/- 8.78%) and parallel squat (28.00 +/- 10.29%), it increased significantly during the full squat (35.47 +/- 1.45%). Similar results were shown for peak values, which displayed significantly greater activity during performance of the full squat as compared to lesser squat depths.
As opposed to the GM, squat depth has little effect on hamstrings involvement. Maximum hamstrings activity tends to occur between 10 to 70 degrees of flexion (Escamilla, et al., 1998; Wilk, et al., 1996, Signorile, et al., 1994), but the magnitude of variation in peak and mean torque is not significant between partial squats, parallel squats and full squats. This is consistent with the bi-articular structure of the muscle complex. Since the hamstrings function both as hip extensors and knee flexors, muscle length remains fairly constant throughout performance, providing a relatively even force output.
Muscular forces at the knee are largely produced by the quadriceps femoris, with muscle activity peaking at approximately 80 to 90 degrees of flexion and remaining relatively consistent thereafter (Escamilla, et al., 1998; Wilk, et al., 1996). This would seem to infer that squatting past 90 degrees is superfluous if the goal is to maximize quadriceps development.
In conclusion, there is scant evidence to show that deep squats are contraindicated in those with healthy knee function. The decision as to how low to squat should therefore be based on an individual’s performance-oriented goals and considered in conjunction with any pathological issues that may be apparent. Those with PCL disorders should refrain from squatting below 50 to 60 degrees until the injury is fully healed. Disorders such as chondromalacia, osteoarthritis, and osteochondritis may also contraindicate the performance of deep squats. To optimize development of the gluteus maximus, squats should be carried out through their full range of motion; to target the quadriceps femoris, a squat depth of 90 degrees appears to be optimal.
Article from http://www.lookgreatnaked.com
Caterisano A, Moss RF, Pellinger TK, Woodruff K, Lewis VC, Booth W, Khadra T. (2002). The effect of back squat depth on the EMG activity of 4 superficial hip and thigh muscles. Journal of Strength and Conditioning Research, 16(3), 428-32.
Chandler, T., Wilson, G., Stone, M. (1989). The effect of the squat exercise on knee stability. Medicine and Science in Sports and Exercise, 21(3). 299-303.
Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE, Andrews JR. (1998). Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises, Medicine & Science in Sports & Exercise, 30, 556-569.
Escamilla R.F. (2001). Knee biomechanics of the dynamic squat exercise. Medicine and Science in Sports and Exercise, 33, 127-141.
Escamilla RF, Fleisig GS, Zheng N, Lander JE, Barrentine SW, Andrews JR, Bergemann BW, Moorman CT. (2001). Effects of technique variations on knee biomechanics during the squat and leg press. Medicine and Science in Sports and Exercise, 33, 1552-1566.
Kanamori A, Woo SL, Ma CB, Zeminski J, Rudy TW, Li G, Livesay GA. (2000). The forces in the anterior cruciate ligament and knee kinematics during a simulated pivot shift test: A human cadaveric study using robotic technology. Arthroscopy, 16(6), 633-9.
Klein, K. (1961). The deep squat exercise as utilized in weight training for athletes and its effects on the ligaments of the knee. JAPMR, 15(1), 6-11
Li G, Zayontz S, DeFrate LE, Most E, Suggs JF, Rubash HE. (2004). Kinematics of the knee at high flexion angles: an in vitro investigation. Journal of Orthopaedic Research, 27(6), 699-706
Li G, Zayontz S, Most E, DeFrate LE, Suggs JF, Rubash HE. (2004). In situ forces of the anterior and posterior cruciate ligaments in high knee flexion: an in vitro investigation. Journal of Orthopaedic Research, 22(2), 293-7
Li G, Rudy TW, Sakane M, Kanamori A, Ma CB, Woo SL. (1999). The importance of quadriceps and hamstring muscleloading on knee kinematics and in-situ forces in the ACL. Journal of Biomechanics, 32(4), 395-400
Markolf KL, Slauterbeck JL, Armstrong KL, Shapiro MM, Finerman GA. (1996) Effects of combined knee loadings on posterior cruciate ligament force generation. Journal of Orthopaedic Research, 14 (4), 633-8
Meyers, E. (1971). Effect of selected exercise variables on ligament stability and flexibility of the knee. Research Quarterly, 42(4), 411-422.
Nisell R, & Ekholm J. (1986). Joint load during the parallel squat in powerlifting and force analysis of in vivo bilateral quadriceps tendon rupture. Scandinavian Journal of Sports Sciences, 8, 63-70.
Panariello, R., Backus, S., Parker, J. (1994). The effect of the squat exercise on anterior-posterior knee translation in professional football players. American Journal of Sports Medicine, 22(6), 768-773.
Sakane M, Fox RJ, Woo SL, Livesay GA, Li G, Fu FH. (1997). In situ forces in the anterior cruciate ligament and its bundles in response to anterior tibial loads. Journal of Orthopaedic Research, 15 (2), 285-93
Signorile JF, Weber B, Roll B, Caruso John, Lowensteyn I, Perry AC. (1994) An electromyographical comparison of the squat and knee extension exercises. Journal of Strength and Conditioning Research, 8, 178-183.
Steiner, M., Grana, W., Chilag, K., Schelberg-Karnes, E. (1986). The effect of exercise on anterior-posterior knee laxity. American Journal of Sports Medicine. 14(1), 24-29.
Wilk KE, Escamilla RF, Fleisig GS, Barrentine SW, Andrews JR, Boyd ML. (1996). A comparison of tibiofemoral joint forces and electromyographic activity during open and closed kinetic chain exercises. American Journal of Sports Medicine, 24 (4), 518-27.


